Evaluation of an Ovarian Mass: Why Age Matters | Case-Based Guide
Patient age is one of the strongest predictors of the biology of an ovarian mass and should guide the differential diagnosis, tumour marker selection and management
Learning Objectives
After reading this article, you should be able to:
- Explain why patient age is one of the strongest predictors of the underlying pathology of an ovarian mass.
- Develop an age-appropriate differential diagnosis.
- Select tumour markers based on the patient’s age and the likely pathology.
- Understand how age influences subsequent management.
Clinical Case
A 17-year-old girl presented to her family physician with intermittent lower abdominal pain for three months. The pain was dull, non-radiating and unrelated to her menstrual cycle. She had also noticed mild abdominal fullness. There was no nausea, vomiting, change in bowel habits, urinary symptoms or weight loss.
She attained menarche at 12 years of age and had regular menstrual cycles. There was no history of precocious puberty, virilisation or endocrine symptoms.
Pelvic ultrasonography demonstrated a 7 cm predominantly cystic left ovarian mass with a thin wall and no obvious solid nodules. There was no ascites. The right ovary and uterus appeared normal.
She was referred to a gynaecologist for further evaluation.
The immediate question was straightforward:
Could this be ovarian cancer?
Why Age Matters in the Evaluation of an Ovarian Mass
Two patients may have identical ultrasound findings but completely different diseases.
Patient age changes the probability of different ovarian tumours. Consequently, the same imaging appearance may lead to a different differential diagnosis, a different choice of tumour markers and a different management strategy.
Understanding this relationship between age and tumour biology is one of the most useful principles in gynaecologic oncology.
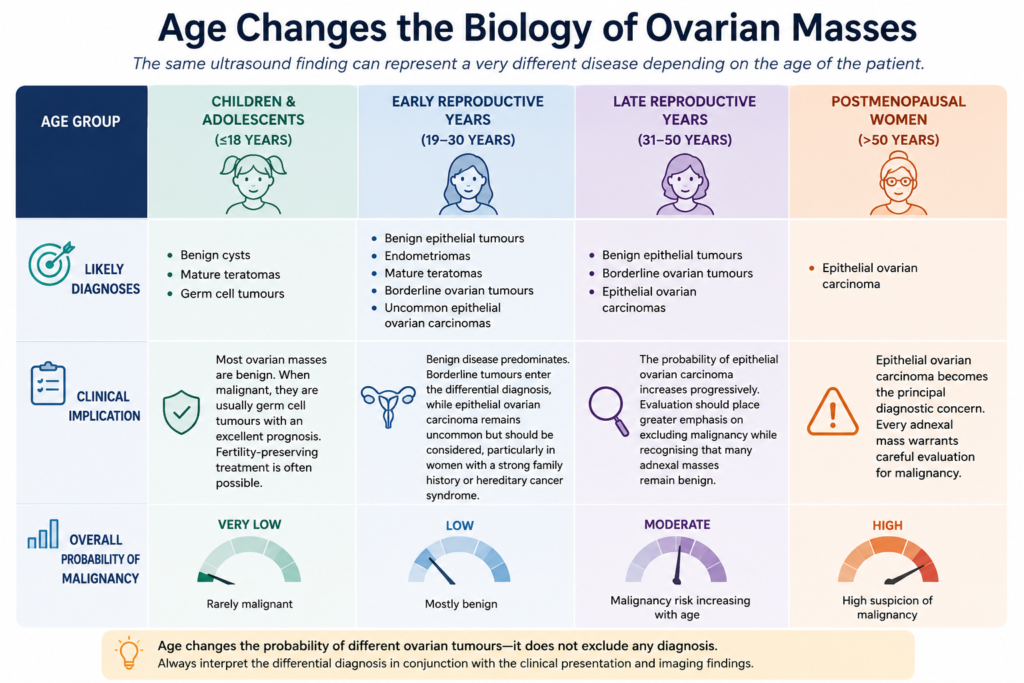
How Ovarian Tumour Biology Changes with Age
Before interpreting an ovarian mass, consider the patient’s age. The figure below illustrates how the spectrum of ovarian tumours changes across a woman’s lifetime and explains why the same ultrasound finding may have a very different differential diagnosis in different age groups
Applying Age-Based Evaluation to Our Patient
Our patient is 17 years old. Based on her age (Figure 1), the leading differential diagnoses are a benign epithelial cystadenoma, a mature cystic teratoma and, less commonly, a malignant germ cell tumour. Invasive epithelial ovarian carcinoma is considerably less likely than it would be in an older woman.
The ultrasound demonstrated a thin-walled predominantly cystic lesion without mural nodules or ascites. These features further reduced the likelihood of invasive epithelial ovarian carcinoma and favoured a benign ovarian neoplasm.
Neither age nor imaging establishes the diagnosis independently. Together, they guide selecting appropriate investigations and planning management.
Tumour Markers in the Evaluation of an Ovarian Mass
The tumour marker panel should reflect the patient’s age and the pathology that is most likely at that age.
In children and younger adolescents, evaluation focuses primarily on AFP, β-hCG and LDH, reflecting the predominance of germ cell tumours.
By late adolescence and early adulthood, epithelial tumours also enter the differential diagnosis. Consequently, a 17-year-old with an adnexal mass will usually undergo evaluation with AFP, β-hCG, LDH and CA-125. Additional markers, such as inhibin, may be requested when a sex cord-stromal tumour is suspected.
As women age, epithelial ovarian carcinoma becomes increasingly common, and CA-125 assumes greater importance in the diagnostic work-up.
The investigation should always reflect the patient’s age and the tumour biology that is most likely at that age.
Returning to the Case
MRI confirmed a thin-walled cyst arising from the left ovary without mural nodules, papillary projections or ascites. Serum AFP, β-hCG, LDH and CA-125 were all within normal limits.
Taken together, the patient’s age, imaging findings and tumour markers strongly favoured a benign ovarian neoplasm.
The patient underwent fertility-preserving laparoscopic ovarian cystectomy.
Histopathological examination confirmed a benign serous cystadenoma.
She made an uneventful recovery with preservation of normal ovarian tissue.
Why Was Surgery Recommended?
Current guidelines recommend specialist assessment and consideration of surgery for ovarian masses that are:
- Persistent on follow-up.
- Symptomatic.
- Complex on imaging.
- Suspicious for malignancy.
Conversely, conservative management with interval follow-up is appropriate when the clinical presentation and imaging are reassuring, symptoms are minimal, and there are no features suggesting malignancy or ovarian torsion.
Application to this case: Although imaging and tumour markers strongly suggested a benign ovarian neoplasm, the patient remained symptomatic and had a persistent 7 cm ovarian mass. Fertility-preserving laparoscopic cystectomy therefore provided both definitive diagnosis and treatment while preserving ovarian function.
Now Change Only One Variable
Imagine that the ultrasound findings were identical.
The cyst is still 7 cm.
It is still predominantly cystic.
There is still no ascites.
Only one fact changes.
The patient is now 65 years old.
Would your differential diagnosis remain the same?
Almost certainly not.
Age alone substantially increases the probability of epithelial ovarian carcinoma. The investigation would place greater emphasis on CA-125, careful assessment for malignant ultrasound features and early referral to a gynaecologic oncology service.
The ultrasound has not changed. The biology has.
Common Pitfalls
- Equating cyst size with malignancy. Large ovarian cysts are not necessarily malignant. Some of the largest ovarian masses are benign or borderline mucinous tumours
- Using the same tumour marker panel for every patient regardless of age.
- Ignoring patient age when interpreting ultrasound findings.
Clinical Pearls
- Patient age is one of the strongest predictors of the underlying biology of an ovarian mass.
- Most ovarian masses in adolescents are benign. When malignant, they are usually highly curable germ cell tumours.
- Select tumour markers according to the patient’s age and the most likely diagnosis.
- Always interpret ultrasound findings in the context of the patient’s age.
References
Meys EM, Kaijser J, Kruitwagen RF, Slangen BF, Van Calster B, Aertgeerts B, Verbakel JY, Timmerman D, Van Gorp T. Subjective assessment versus ultrasound models to diagnose ovarian cancer: A systematic review and meta-analysis. Eur J Cancer. 2016 May;58:17-29. doi: 10.1016/j.ejca.2016.01.007..
American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology. Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses. Obstet Gynecol. 2016 Nov;128(5):e210-e226. doi: 10.1097/AOG.0000000000001768